

Introduction
Materials and Methods
Participants
Experimental Procedure
Horticultural Activity Program Design
Instruments and Measurements
Data Analysis
Results and Discussion
Pre-Homogeneity Test Between Groups Before Conducting the Horticultural Activity Program
Changes of Stress Index Through Autonomic Nerve Measurement
Changes in Vascular Health Index and Mean Heart Rate
Introduction
Cerebrovascular disease is one of the three major causes of death along with cancer and heart disease worldwide (WHO, 2014). In Korea, there are 77 deaths due to cerebrovascular disease per 100,000 people, making it the third leading cause of death (Statistics Korea, 2016). Cerebrovascular disease, often referred to as stroke, occurs abruptly, is accompanied by loss of normal neurological function, and progresses rapidly within a short period of time. Depending on the area of brain injury, it causes various complex dysfunctions, such as impaired motor function and loss of sensation and balance (Busse, 2003; Glen, 2006). Because of various risk factors and uncertain prognosis, the individual’s life itself becomes unbalanced and they experience physical as well as mental stress (Park, 2001).
The presence of green plants in a residential environment is effective in relieving technostress, as measured by blood pressure, pulse, electrocardiogram, and eye fatigue, and viewing plants stabilizes people mentally and physiologically (Son and Lee, 1997). In England, Lowry (2007) studied soil to see if it makes people feel happy and revealed the correlation between the soil bacteria Mycobacterium vaccae and mental health of humans. M. vaccae enters the human body through the respiratory tract and is released into the stressed brain, increasing the secretion of serotonin, which helps people feel happy and be more resistant to stress (Seoul news paper, 2010). In Korea, however, hospitals have prohibited people from bringing plants into patient rooms because of the presence of pathogenic microorganisms in the soil, and horticultural activities involving plant cultivation and crafts that do not touch soil are also less common than horticultural activities that touch soil (Jang et al., 2017).
However, from the results of a study conducted in the same environmental conditions as the hospital, no pathogenic microorganisms were detected in the plant soil (Yun et al., 2018). Horticultural activities used as mediators of alternative therapies include active horticultural activities and passive horticultural activities (Yun, 2007). In this study, active horticultural activities in the hospital were divided into those that touch the soil and those that do not touch the soil. Passive horticultural activities were conducted by observing the plants planted in the soil and examining the physiological changes of the emotional functions. The purpose of this study was to determine if horticultural activities can be used as a therapeutic tool for patients.
Materials and Methods
Participants
The subjects were selected as those with cognitive function MMSE-K (Mini Mental State Examination-Korean) of 20 or more patients admitted to B rehabilitation hospital in G city, Gyeongsangbuk-do, with cerebrovascular diseases such as stroke, cerebral hemorrhage, cerebral infarction, and dementia. The subject was informed of the purpose of the study and stated their intention to participate. The final study consisted of 53 patients with brain disease participating in the program 100%. The control group consisted of 12 patients (8 male and 4 female), the horticultural activity experimental group that touched the soil consisted of 16 patients (all female), the horticultural activity experimental group that did not touch the soil consisted of 15 patients (4 male and 11 female), and the experimental group that only watched the plants in the hospital room consisted of 10 patients (5 male and 5 female).
Experimental Procedure
The participants in the study were divided into the control group and the three experimental groups (horticultural activity group touching the soil [experimental group A], horticultural activity group not touching soil [experimental group B], and experimental group simply watching the plants in the hospital room [experimental group C]). A true experimental design was conducted for the multiple treatment groups, and the control group and the three experimental groups all had the same pre- and post-test. In the control group, the stress index, the vascular age, and the mean pulse rate were measured without conducting the program after the pre-test, but they were required to only receive the rehabilitation therapy. Experimental groups A and B had active horticultural activity and experimental group C had passive horticultural activity. The experimental groups were required to perform horticultural activities together with rehabilitation therapy; after the pre-test and running the program, the post-test was measured (Table 1).

Horticultural Activity Program Design
This study was conducted from August 2, 2017 to October 18, 2017, once a week for a total of 12 sessions. The horticultural activity program was conducted by the 2nd grade welfare gardener (Korea Horticultural Therapy Welfare Association), two assistant therapists (Completion of Lifelong Education Welfare and Gardening Course Recognized by the Korea Horticultural Therapy Welfare Association), and a social worker. Patients with brain disease suffer from severe stress just maintaining their daily lives and need the help of others (Moon et al., 2004). The purpose of this study was to lower the stress index of patients with brain disease through horticultural activities. For each session, one of the words “happiness,” “health,” and “hope” was written on the name tag and put on the result of the work. The same plants were selected to be used in the three experimental groups. According to Jang’s (2016) study of gardening activities using soil, the plants were selected in ascending order of frequency of use and applied at each session. The horticultural activity program was designed by dividing horticultural activities into active horticultural activities (activities that touch the soil and activities that do not touch the soil) and passive horticultural activities (plants placed in the room). Also, experimental group A, which included patients who had no objection to touching the soil, was allowed to touch the soil with their hands, and experimental group B did not touch the soil. Experimental group C had the products of experimental group A in their rooms to be appreciated (Table 2).
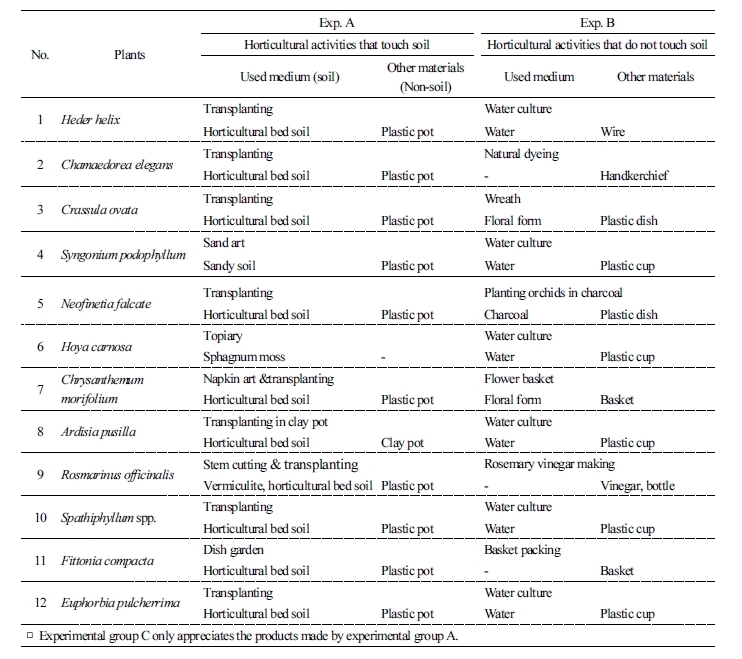
Table 2. Plant species and horticultural activity programs performed in experimental groups A and B (Continued) 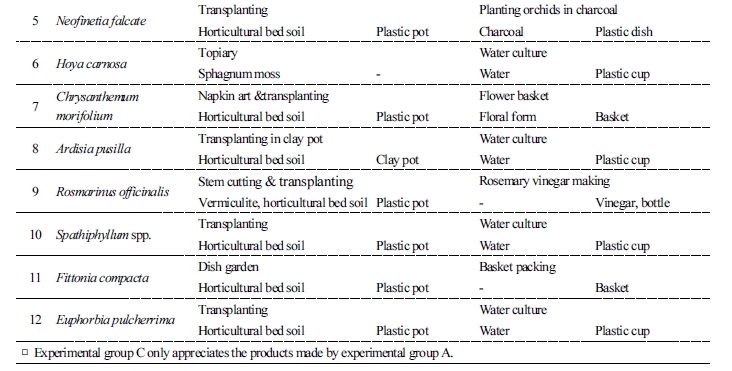 |
Instruments and Measurements
Autonomic stress measurement: uBioMacpa v70 (BioSense Creative, Korea) was used to measure autonomic stress level. uBioMacpa analyzes heart pulses by measuring pulse waves noninvasively on fingertip capillaries. The degree of stress in the human body, the vascular age, and whether the autonomic nervous system is abnormal can also be checked. The vascular health index was measured by subtracting the vascular age from the age of the patient. Considering that there can be a difference in the measurement results even if there is slight movement, the heart rate variability of the autonomic nervous system was measured 2 min and 150 s when the subject was lying down after the horticultural activity. Pulse is a wave that occurs when the blood that is released from the heart touches the blood vessel wall, and it is repeated by the heartbeat due to the increase and decrease of the blood flow. It is measured through the signal detected by applying light of a specific wavelength to the human body. The uBioMacpa stress measurement is based on the standards provided by the analysis of the average pulse variability signals from the North American Heart Rate Electrophysiology Society and the European Heart Association (Vanderlei et al., 2009).
Data Analysis
Changes before and after the horticultural activity program were analyzed using the SPSS program (version 19.0, IBM, USA) with nonparametric tests. The pre-homogeneity of the control and three experimental groups and the post-intergroup comparison was analyzed by the Kruskal-Wallis test. The change of each factor in the pre- and post-test was analyzed by Wilcoxon signed rank, and the significance level was p < 0.05.
Results and Discussion
Pre-Homogeneity Test Between Groups Before Conducting the Horticultural Activity Program
The homogeneity of the control group, the horticultural activity group touching the soil (experimental group A), the horticultural activity group not touching soil (experimental group B), and the experimental group simply watching the plants in the hospital room (experimental group C) was examined and the results using the Kruskal-Wallis test are in Table 3. Since there was no significant difference in average age (p = 0.198) and MMSE-K (p = 0.293), the stress index (p = 0.131), the vascular health index (p = 0.978), and the average pulse rate (p = 0.485), the groups were considered homogeneous group and the study was carried out.

Changes of Stress Index Through Autonomic Nerve Measurement
The stress index is a numerical value obtained by synthesizing the values of pulse rate variability (pulse diversity), sympathetic activity, parasympathetic activity, autonomic balance, mean pulse, standard deviation of pulse, and average deviation. The results of examining the autonomic nervous stress index of the control and experimental groups using uBioMacpa are presented in Table 4. The stress index of the control group increased from 54.8 to 55.3. However, the stress index of experimental group A decreased from 60.3 to 46.8 (p = 0.001), and that of the experimental group B significantly lowered from 67.3 to 56.7 (p = 0.036). Experimental group C lowered from 65.3 to 54.3 but was not significant (p = 0.214).
The physical disabilities of patients with cerebral diseases, such as stroke, cerebral hemorrhage, and cerebral infarction, can increase psychological stress and cause depression, which reduces quality of life (Berg et al., 2001). Studies have shown that the horticultural activity of planting plants that touch soil helps patients recognize the flow of time according to the changes of the plant, improves cognitive function via the learning of various plant names and using words, reduces stress, and restores psychological health by reducing tension (Talbott and Stern, 1976; Ulrich, 1981).
This suggests that the cortisol content of patients in surgery and inpatients was decreased when plants were placed in their rooms (Jang, 2008), which is consistent with previous results that there is a reduction in human mental stress when looking at green plants or flowers (Goodwin et al., 1994). In particular, as exercise has a special relationship with mental health (Morgan and O’Connor, 1988), increasing the the frequency of physical activity creates more diverse physiological responses such as catecholamine and some peptide hormone secretion, which is an important means of securing mental health Mazzeo, 1991; McGowan et al., 1985). This study also found that it is more effective to actively perform horticultural activities.

Changes in Vascular Health Index and Mean Heart Rate
The results of examining the vascular health index and the mean heart rate of the control group, the horticultural activity group touching the soil (experimental group A), the horticultural activity group not touching soil (experimental group B), and the experimental group simply watching the plants in the hospital room (experimental group C) using uBioMacpa are as shown in Table 5. There was no significant difference in vascular health index between experimental group A (p = 0.091) and experimental group B (p = 0.799), who actively participated in horticultural activities. However, it was found that the vascular health index of the control group decreased from -11.1 to -0.6 (p = 0.010) and that that of the experimental group C also decreased significantly from -13.5 to -0.8 (p = 0.047). In the case of a hemiplegic patient performing the horticultural activity, placing the injured hand on the table even for a short period of time, in a comfortable position holding the pot motionless or helping the hand that is maneuverable, the vascular age is no longer deteriorated by inducing the use of the injured side as well. Exercise directly increases blood flow and increases nitric oxide secretion, and up-regulation of eNOS expression can increase vascular endothelial function (Jungersten et al., 1997). Regular exercise also directly affects vascular remodeling (Naylor et al., 2006). As a result of this study, it was found that the group that directly executed the horticultural activity was more effective than the group that did not perform the horticultural activity.
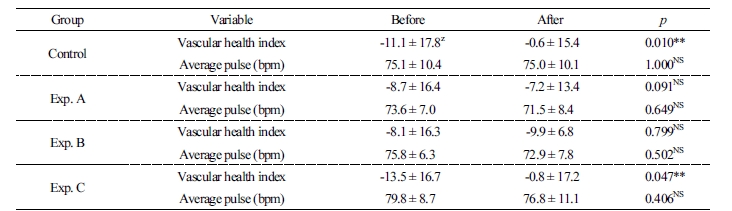
The mean heart rate was not found to show any significant difference between the control group (p = 1.000) and experimental groups A (p = 0.649), B (p = 0.502), and C (p = 0.406), but all of the experimental groups except the control group showed a stable heart rate with the decreased heart rate. Through the physical activity of patients with brain disease, it is thought that the feeling of emotional stability (Relf, 1990) is reflected in the stable average heart rate as negative emotions are diminished and pleasure and achievement are generated. This study supports the results of the previous study that the pulse rates of the elderly decreased after a horticultural therapy program that incorporates recall (Lee et al., 2008), and the heart rate is low when the eagerness to work is given to the task (Ekman et al., 1983).
If a hospital that is a treatment space for people who are not healthy physically and/or mentally does not prohibit the presence of flowers and plants in the rooms due to the increase in workload for the medical staff and manager in the hospital, and if the safety of the soil is verified, and patient-oriented active and positive horticultural activities are introduced, we conclude that it will help not only the improvement of the patients' health but also that of the medical environment.
