

Introduction
Materials and Methods
Results and Discussion
Distribution of Horticultural Activity Intervention Research
Demographics of Horticultural Activity Study Subjects
Characteristics of Horticultural Activity Interventions
Effects of Horticultural Activity Intervention
Therapeutic Effects of Horticultural Activities
Introduction
The broad discipline of the human aspects of horticulture recognizes that horticulture has economic, environmental, and health impacts, all of which improve the quality of life (Relf and Lohr, 2003). The therapeutic role of horticulture has especially been of interest following the use of gardening and farming to improve both mental and physical health after World War II (Matsuo, 1996). The use of horticulture in medicine has been documented as far back as ancient Egypt, when court physicians instructed royalty to walk among the palace gardens as a prescription for mental illness (Simson and Straus, 1998). By the late 1700’s and early 1800’s, the use of horticulture gradually became recognized as an acceptable form of therapy for use in mental health institutions (Shoemaker, 2004). In the early 1900’s, the application of horticulture for therapy was expanded to other populations, including the mentally handicapped, at-risk youth, and war veterans. In addition, the term horticultural therapy was coined, which is defined as “a professional treatment provided by a trained horticultural therapist by using plant and horticultural activities in a program pre-designed with therapeutic goals and purposes to improve physical rehabilitation and mental recovery of clients” (Son et al., 2006). Since the early 2000’s, patients with various ailments have been participating in horticultural therapy programs and horticultural activity programs in many countries, and the use of horticulture for both intervention and treatment has been investigated.
In South Korea, horticultural therapy was first introduced in the 1980s, and the working group that eventually gave rise to the Korean Horticultural Therapy and Well-being Association was established in 1997 (Park et al., 2012a). Since then, this association has been promoting horticultural therapy as a profession and has certified ~2000 horticultural therapists. As a result, horticultural therapy in South Korea has rapidly grown over the past 20 years (Park et al., 2012a), and gardening has become popular in cities after the establishment of legislation for developing and supporting urban agriculture (RDA, 2010). However, although some studies have investigated the health benefits of horticultural activity, no review articles have analyzed the research trends or characteristics of horticultural activity intervention. Therefore, the objective of the present study was to review the current literature on the outcomes of horticultural activity interventions in order to determine research trends and to analyze the characteristics of horticultural activity intervention, such as the ages and numbers of participants, activity types, number of sessions, and intervention durations.
Materials and Methods
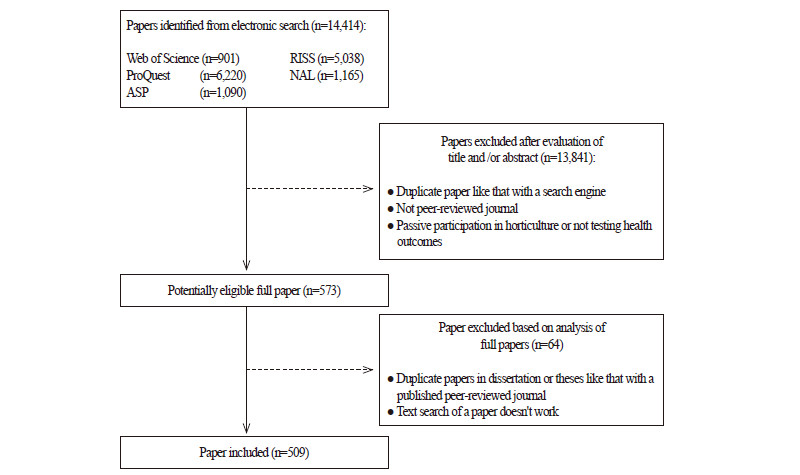
In the present study, we reviewed the literature using search engines such as the Web of Science, Proquest Dissertation and Theses, Academic Search Premier, Research Information Sharing Service, and Korean National Assembly Digital Library to locate journal articles that included relevant search terms (i.e., gardening activity, garden therapy, gardening program, allotment garden, urban agriculture, human issues in horticulture, horticultural therapy, horticultural activity, socio horticulture, and therapeutic horticulture). We initially identified 14,414 journal articles that were published prior to April 2014 and selected 509 of the papers for review by only choosing those that 1) included physical, psychological, social, behavior, cognitive, and educational effects of horticultural activity (e.g., horticultural, gardening, or horticultural therapy programs); 2) were peer-reviewed articles, theses, or dissertations (journal articles were selected when thesis or dissertation research was published); and 3) were written in English or Korean (Fig. 1). Studies that investigated passive participation in horticulture, such as viewing nature or participating in non-structured gardening activities, were excluded.
Results and Discussion
Distribution of Horticultural Activity Intervention Research
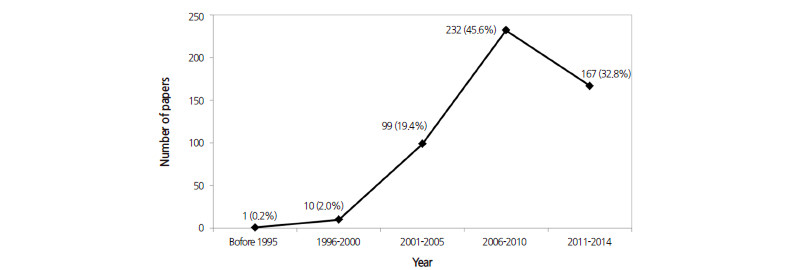
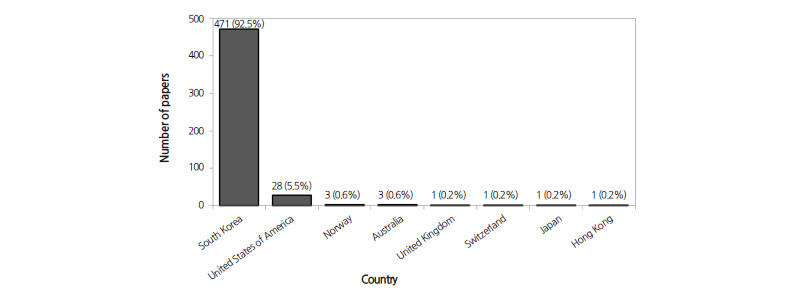
The number of published of research papers on the health benefits of horticultural activity intervention has been increasing since the early 2000’s (Fig. 2). This number increased dramatically from 2006 to 2010, during which 45.6% of the selected papers were published. Horticultural therapy was introduced to South Korea in the 1980’s (Park et al., 2012a) and after 10 years, publication on the topic dramatically increased owing to continued interest and efforts. However, few papers have been published by researchers in other countries. Most of the articles (92.5%) were published by researchers in South Korea, whereas only 5.5% were published by researchers in the US (Fig. 3). The percentage of articles written in Korean and English was 91.7% and 8.3%, respectively.
Demographics of Horticultural Activity Study Subjects
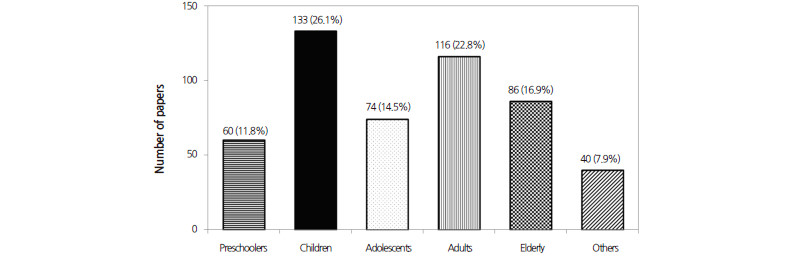
The subjects involved in the 509 investigations reviewed in the present study were classified into several age groups: preschoolers (below 7 years old), children (8 to 13 years old), adolescents (middle and high school students), adults (20 to 64 years old), elderly (over 65 years old), or others (combined age groups) (Fig. 4). Studies that focused on children were the most frequent (26.1%), followed by those that focused on adults (22.8%). Only 16.9% of studies focused on elderly subjects, 14.5% on adolescents, and 11.8% on preschoolers. In most of the studies, the subjects who participated in the gardening intervention were of the same type. Only a few studies (7.9%) combined age groups, such as those that included intergenerational subjects, children and disabled children, and parents and their children.
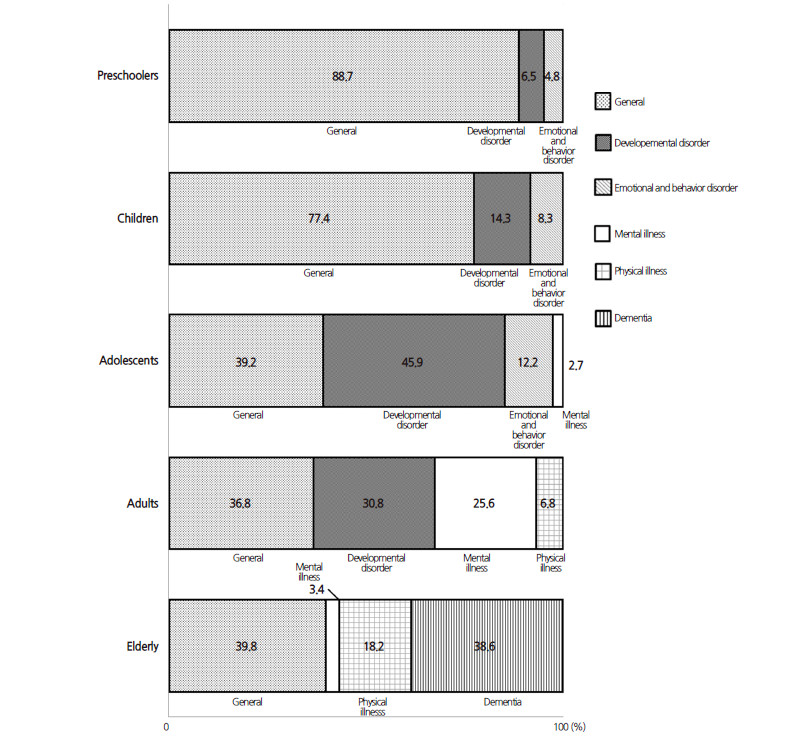
In addition, the studies were also categorized based on the conditions of the subjects (Fig. 5) into one of the following: general, developmental disorders, physical illness, mental illness, emotional and behavioral disorder, or dementia. Subjects without any physical or psychological disease or symptoms were classified as “general” subjects. We found that studies with young subjects, such as those involving preschoolers and children, mainly focused on general subjects without any diseases or disorders, and the horticultural activity interventions were usually managed as regular school or after-school programs. In the case of adolescents and adults, most of the studies involved general subjects or those with developmental disorders. In the case of adults, a large number of studies also involved subjects with mental illness (25.6%), and in the case of adolescents, the horticultural activity interventions were mainly managed as after-school programs or as special classes for disabled students. In the studies that focused on elderly subjects, most focused on either general subjects (39.3%) or subjects with dementia (38.6%). The extension of the national system for supporting therapeutic programs in South Korea to facilities such as day care centers for the elderly with dementia is thought to have increased access to this population.
| |
Fig. 5. Health conditions of subjects treated in the 509 studies reviewed in the present study. General subjects were defined as those without any diseases or disorders. | |
Characteristics of Horticultural Activity Interventions
Types of horticultural activity interventions: The types of horticulture activities used in each intervention were classified as follows: gardening outdoors, planting indoors, making crafts with live plants, arranging flowers, making crafts with artificial or pressed flowers, and “other activities”, including cooking, art, exhibition, field trips, watching audiovisual documents, and so on (Table 1). Most of the horticultural activity interventions were treated as combined activities for all types of subjects. For example, most horticultural activity interventions involving preschoolers were conducted as combined activities, such as the combination of gardening outdoors with other activities (37.5%) or a combination of planting indoors, making crafts with live plants, arranging flowers, making crafts with artificial or pressed flowers, and other activities (14.3%; Table 1). For other subjects, such as adolescents, adults, and the elderly, interventions that combined the six types of activities were used, and interventions that used gardening alone were only conducted in studies that involved preschoolers (16.1%) and children (12.4%).
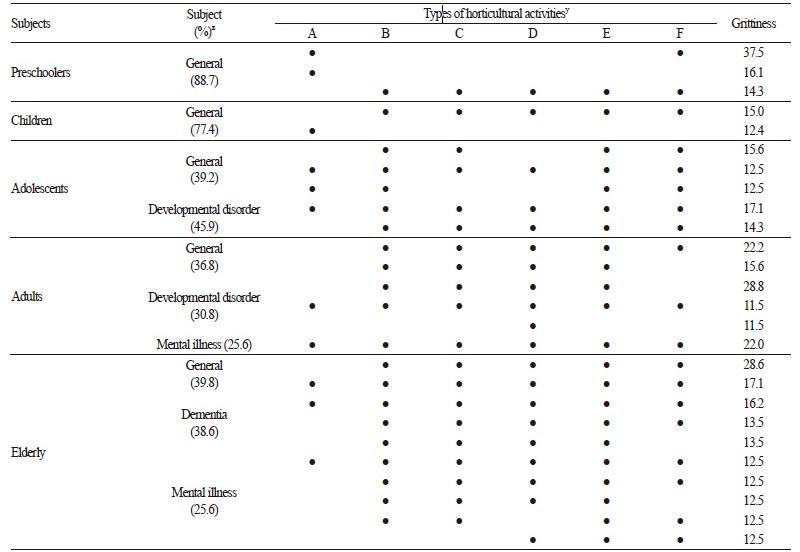
The specific horticultural activities used in gardening interventions might have been determined by the preference of the subjects, as well as logistical factors, such as the available facilities and budgetary constraints. Some studies investigating the preferences of subjects for horticultural activities showed that some subjects enjoyed a combination of horticultural activities more than a single horticultural activity. For example, elderly stroke patients preferred working with live plants, planting transplants, arranging flowers, and sowing seeds (Park et al., 2015). Moreover, if a facility did not have a garden plot for the intervention, only indoor horticultural activities could be used. However, developing a general rule of thumb for selecting activities for specific intervention programs should be avoided, since the therapeutic effects of individual activities remain to be determined.
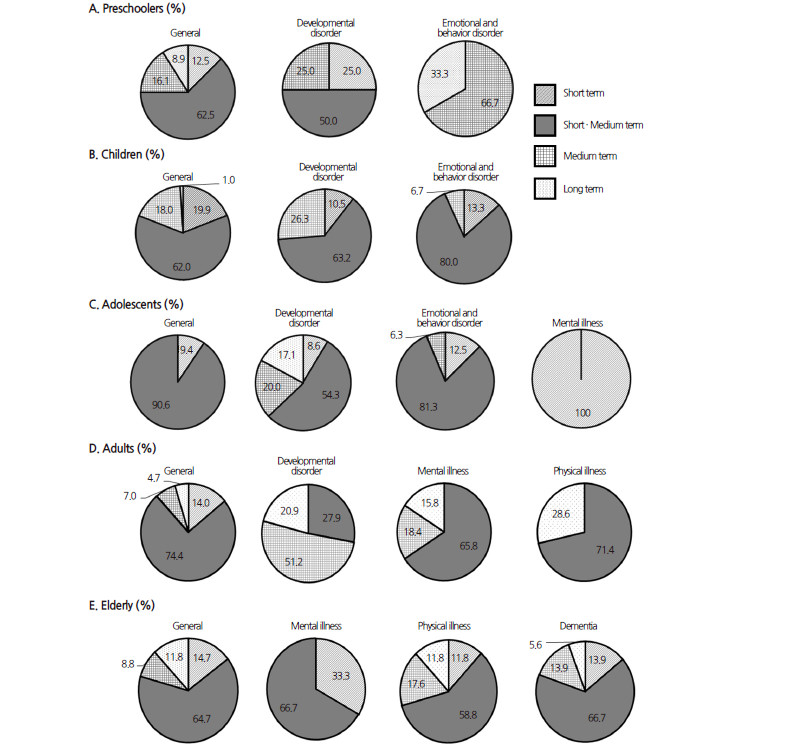
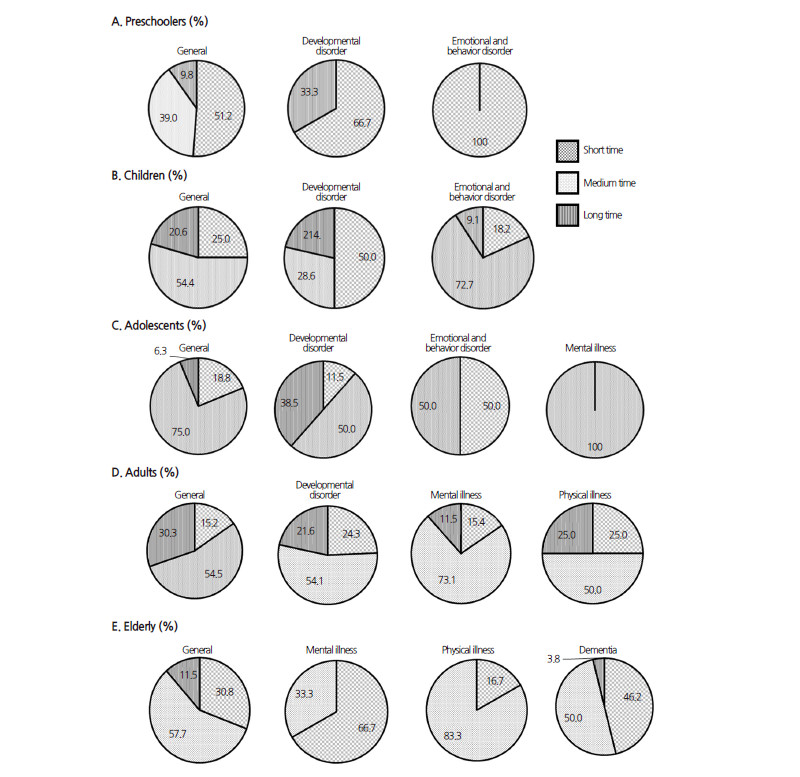
Number of session of horticultural activity interventions: The number of session of horticultural activity interventions were classified as short term (less than 10 sessions for a program), short/medium term (11 to 20 sessions), medium term (21 to 30 sessions), and long term (more than 31 sessions), and the time required for each session was classified as short (> 30 min to 60 min), medium (> 60 min to 120 min), and long (> 120 min), with different subject categories. Short/medium-term interventions were the most frequent (Fig. 6), including 62.5% of preschooler studies, 62% of children studies, 90.6% adolescent studies, 74.4% adult studies, and 64.7% of elderly studies. Most interventions were of medium duration (> 60 min to 120 min), including those for children (54.4%), adolescents (75%), adults (54.5%), and elderly subjects (57.7%), but not preschoolers (Fig. 7). Meanwhile, programs for preschoolers (i.e., general, developmental disorder, and emotional and behavioral disorder), children with developmental disorders, and elderly subjects with mental illness were usually involved in short-term interventions (Fig. 7), probably because these subjects had lower attention levels than the subjects of mediumand long-term interventions.
| |
Fig. 7. Time required per session of horticultural activity intervention. Short time, 30 min to < 60 min; Medium time, 60 min to < 120 mn;i Long time, ≥ 120 min. | |
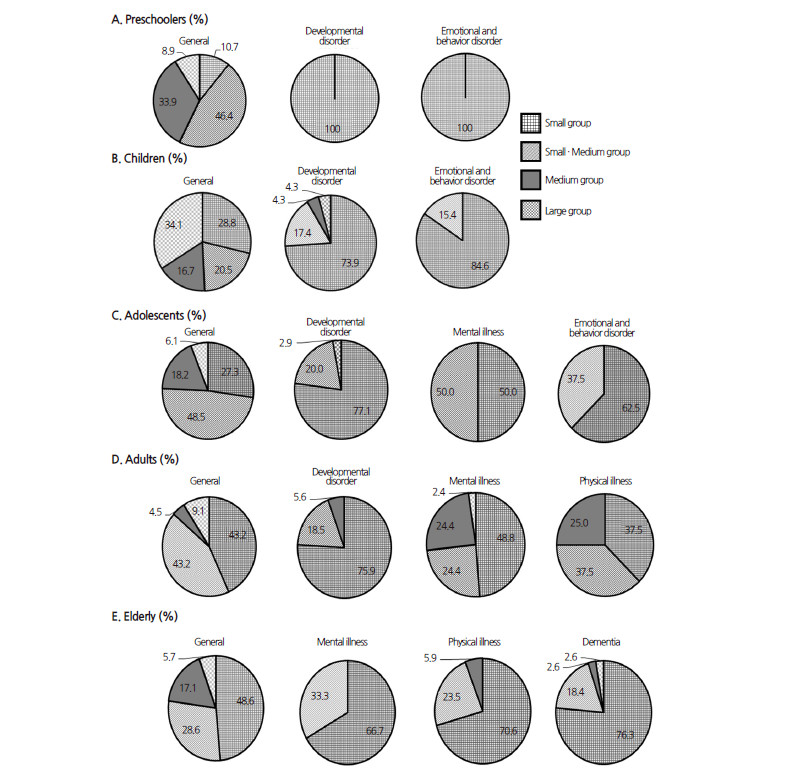
Number of participants in horticultural activity interventions: The sizes of groups participating in the interventions (i.e., number of participants) were classified as small (fewer than 11 subjects), small/medium (11 to 20 subjects), medium (21 to 30 subjects), and large (more than 30 subjects) (Fig. 8). Regardless of age, most of the subjects with diseases or disorders were treated in small groups, whereas the group sizes of the general subjects varied and differed by age. Logistically, it is difficult to conduct a horticultural activity intervention with a medium or large group of young or disabled subjects. Meanwhile, 34.1% of the interventions involving general children treated large groups (i.e., > 31 subjects) at the same time. Korean elementary school classes usually comprise 25-30 students, and most horticultural activity interventions were managed as study units.
| |
Fig. 8. Group size of horticultural activity interventions. Small group, < 11 subjects; Small/Medium group, 11-20 subjects; Medium group, 21-30 subjects; Large group, > 30 subjects. | |
Effects of Horticultural Activity Intervention
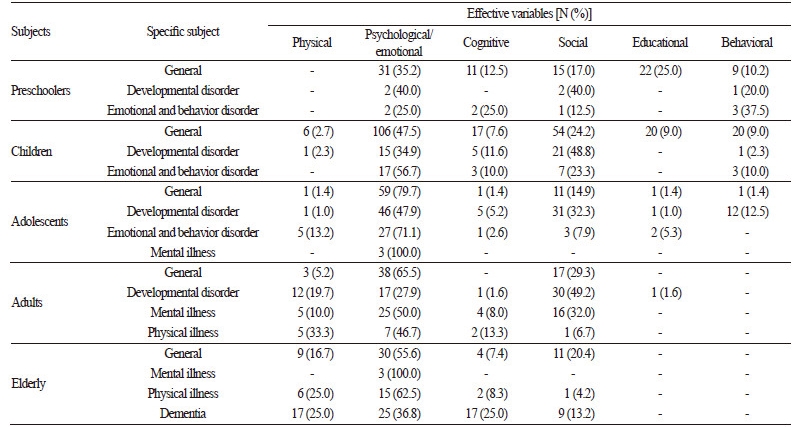
The effects of horticultural activity interventions that were examined in the selected studies could be classified as physical, psychological or emotional, social, behavioral, cognitive, or educational. The most frequently studied variable was a psychological or emotional aspect, although the percentages varied by subject age (Table 2).
Preschoolers and children: Studies of preschoolers mainly included subjects without any diseases or symptoms; 35.2% of these studies investigated the psychological or emotional effects of horticultural activity intervention, such as emotional intelligence and eco-friendly attitude (Table 2). Moreover, 25% of the studies investigated the educational effects of horticultural activity intervention, such as scientific attitudes and scientific investigation ability. In studies of children without any diseases or disorders, 47.5% investigated psychological or emotional effects, such as self-esteem and emotional intelligence, and 24.2% of studies focused on social effects.
In modern society, young and older children do not have sufficient opportunities to experience nature (Kim, 2010) owing to the use of artificial educational materials and increased indoor activities, such as studying and playing computer games (Greenman, 1993; Johnson et al., 2005). Exposure to nature helps enrich children’s emotions and leads to improved emotional intelligence, which is defined as the capacity of individuals to recognize the emotions of themselves and others, to discriminate between different feelings, to label feelings appropriately, and to use emotional information to guide thinking and behavior (Kim, 2005; Mayer and Salovey, 1997). The development of emotional skills during early childhood is crucial for holistic human development (Denham, 1991). Direct exposure to nature by cultivating plants or participating in other activities involving plants is effective for improving emotional health while helping participants experience fun and rewarding activities (Chiang et al., 2007; Kim, 2002a; Lee, 2003).
Regarding the psychological or emotional aspects of treatment, 25 five-year-old children participated in a 14-session horticultural activity intervention that consisted of both indoor and outdoor planting activities, with the purpose of experiencing the plant life cycle by growing plants by themselves (Jeong et al., 2009). The program was conducted once or twice per week, with an average duration of 30–40 min per session, leading to significant improvements in emotional intelligence, environmental attitude, scientific attitude, and exploration ability (Jeong et al., 2009). Choi et al. (2012) conducted an 18-week horticultural activity program that included making a garden plot, planting flowers and vegetables, observing growing plants, harvesting, and produce tasting for 35 preschoolers, who subsequently experienced significant improvements in both emotional intelligence and happiness. Similarly, Nam et al. (2010) reported that 73 elementary school students who participated in a 12-session nature program experienced significantly improved self-esteem and sociability.
Gardening activities provide experience with live plants, which helps children have a serious view of life. Moreover, working with a peer group can provide opportunities for learning collaboration and patience (Matsuo, 1996; Relf, 1992). The extended application of horticultural activity programs for preschoolers and children would be a valuable investment for creating a healthier society.
Adolescents: Most of the studies that focused on general adolescents investigated psychological or emotional effects (79.7%) such as stress and depression, whereas studies that focused on adolescents with developmental disorders investigated psychological or emotional effects (47.9%) such as self-esteem and social effects (32.3%), e.g., personal relationships, social behaviors, and attitude for participation (Table 2). During adolescence, most youth are very sensitive and emotionally conflicted (Kim, 2001), which creates problems for families and schools (Kim, 2002b). In addition, Koreans study many hours for entrance exams, which may lead to depression, stress, and low self-esteem (Kang, 2007).
Among selected studies, Son et al. (2013) reported that 15 female high school students who participated in a 15-session flower arrangement program experienced significantly reduced levels of stress and anxiety, and Shon et al. (2011) reported that 15 male middle school students experienced significant improvements in stress and academic motivation after a 12-session horticultural activity program that included flower arrangement, planting, and making crafts with live plants. Furthermore, a 22-session horticultural therapy program that examined the effects of hydroponics on the work adjustment skills of students with intellectual disabilities improved motor performance, emotional behavioral strategies, and interpersonal negotiation strategies (Joo et al., 2012).
Adults: Of the studies that focused on adults without any diseases or disorders, most investigated psychological or emotional effects (65.5%), such as stress, depression, and self-esteem, or social effects (29.3%), such as personal relationships and sociality (Table 2). In addition, studies that focused on adults with developmental disorders investigated social effects (49.2%), such as personal relationships, social skills, and adaptive behavior, or psychological or emotional effects (27.9%), such as self-esteem or behavior characteristics. Studies of adults with mental illness examined psychological or emotional effects (50%), such as depression and self-esteem, or social effects (32%), such as personal relationships, sociality, and social behavior.
In cities, menopausal married women who had problems with stress, anxiety, and depression (Lee and Choi, 1992; Washington, 1999) experienced significant reductions in anxiety and depression and improved life satisfaction after participating in a 12-session horticultural activity program that included indoor planting, arranging flowers, and making crafts with live plants (Kim et al., 2012). Another 24-session horticultural therapy program was shown to significantly improve the social skills, interpersonal relationships, and self-esteem of 12 intellectually disabled women (Kim et al., 2008). Thus, this program would be useful as a rehabilitation program for helping intellectually disabled women fit into society by improving their interpersonal relationships and socialization.
Elderly: Most studies that focused on elderly subjects without any diseases or disorders investigated psychological or emotional effects (55.6%), such as self-esteem, life satisfaction, and depression, or social effects (20.4%), such as social support and personal relationships (Table 2). Studies of elderly subjects with dementia investigated the following: psychological or emotional effects (36.8%), such as depression; physical effects (25%), such as the functioning of upper extremities, hand functional ability, and activities of daily living; or cognitive effects (25%), such as cognitive function.
In one study, 12 elderly subjects from a welfare center reported significantly improved self-esteem and social support after participating in a 15-session horticultural activity program that included planting, making crafts with live plants, and pressing flowers (Oh and Yoo, 2010). In another study, 12 elderly subjects with dementia showed significantly reduced symptoms of depression and increased self-esteem after participating in a 12-session horticultural therapy program that included planting, flower arrangement, and making crafts with live plants (Lee et al., 2007), and a 20-session horticultural therapy program was shown to significantly improve the cognitive and upper extremity functions of elderly subjects with dementia (Song, 2007). Although few studies have focused on subjects with emotional and behavioral disorders, mental illness, or physical illness, psychological or emotional and social effects were mainly reported in these studies (Table 2).
Therapeutic Effects of Horticultural Activities
The research articles selected in the current study reported that horticultural activities had positive effects on the psychological health of subjects. The positive effects of green plants and natural environments have been reported previously. For example, Ulrich (1983) reported that natural environments reduce negative emotions from stress and activate the sympathetic nervous system. In addition, patients recover more quickly from surgery and experience reduced stress levels after exposure to natural environments (Ulrich, 1984; Ulrich et al., 1991). Kaplan and Kaplan (1989) proposed the notion that humans recognize nature or green scenery without requiring sophisticated thinking, which releases mental fatigue. Moreover, humans recover more rapidly in a green, natural setting than in urban scenery (Kaplan, 1987). Ikei et al. (2014) reported that green plants stabilize the autonomic nervous system in indoor environments by activating the parasympathetic nervous system. Moreover, Lee et al. (2015) reported that working with plants could have a stabilizing effect by activating the parasympathetic nervous system. Although more research is needed on the therapeutic mechanisms of horticultural activities for psychological well being, green or natural environments clearly have positive effects on the sympathetic nervous system, leading to emotional stability.
Various common horticultural activities are considered to represent low- to high-intensity physical activities in various populations (Park et al., 2011, 2012b, 2013a, 2014a, 2014b). Regular physical activity has been reported to control or prevent chronic diseases (ACSM, 1998). Therefore, similar health benefits could be expected from participating in horticultural activity interventions or horticultural therapy programs. Moreover, horticultural activities and the movements associated with flower arranging use muscles of both the upper and lower limbs, as well as muscles of the hand (Lee et al., 2012; Park et al., 2013b, 2014c), and weight-bearing activities can improve muscle strength, physical ability, and bone mineral density.
Working in a garden with friends, colleagues, or family members also provides an opportunity to improve life skills, such as teamwork, cooperation, accomplishment of goals, self-confidence, self-expression, and the ability to accept the decisions of others (Choi, 2007; Kim, 2006; Song, 2002; Song, 2008; Yoon, 2001). Kim et al. (2014) reported that 123 elementary school students experienced improved peer relations, peer stature, and sociality after participating in 10 weekly sessions of gardening intervention. Gardening also provides enjoyment and fun; continuous participation in gardening represents part of a physically active lifestyle. Park et al. (2008) reported that older Americans gardened for an average of 33 hours per week in May and for almost 15 hours in June and July, which greatly contributed to their physically active lifestyle. Moreover, gardening provides hands-on experience with the process of growing plants and provides an opportunity to observe the life cycle and seasonal variations of plants (Park et al., 2008) and the ecosystem (Montessori, 1964; Morris et al., 2000).
In conclusion, studies focused on children were the most frequent, followed by those focused on adults; however, elderly, adolescent, and preschooler subjects were also treated. Interventions for younger subjects, such as preschoolers and children, were mainly intended for general subjects (i.e., without any diseases or disorders). The various types of horticultural activities, such as gardening outdoors, planting indoors, making crafts with live plants, arranging flowers, making crafts with artificial or pressed flowers, and other activities were usually combined. Short/medium term interventions (11 to 20 sessions) were the most frequent, and the average duration of interventions for children, adolescents, adults, and elderly subjects ranged from 60 min to <120 min. Programs for preschoolers (general, developmental disorder, and emotional and behavioral disorder), children with developmental disorders, and elderly subjects with mental illness were usually conducted for shorter durations. In the case of preschoolers and adolescents without any diseases or disorders, the interventions were conducted with groups of 11–20 subjects. Subjects with diseases or disorders, such as developmental disorders, emotional and behavioral disorders, mental illness, and physical illness, were treated in smaller groups, whereas 34.1% of the interventions for general children treated large groups of over 31 subjects at a time. In addition, we found that most of the studies investigating the psychological or emotional effects of horticultural intervention, such as emotional intelligence, self-esteem, stress, and depression, and social aspects, such as sociality, personal relationships, and social behavior were considerably focused. Future studies are needed to analyze the research methodology, specific outcomes, and strengths or weaknesses of research about horticultural activity interventions.
